 CASE DISCUSSIONCASE DISCUSSION
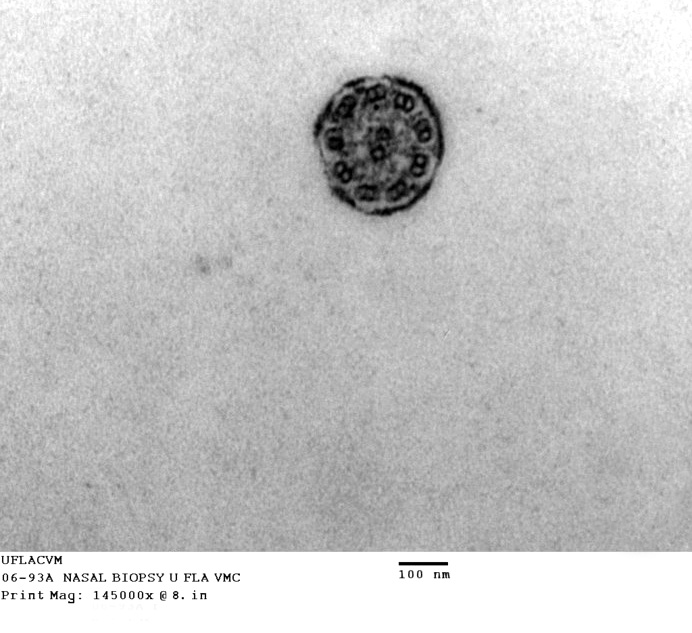
CASE DISCUSSIONCASE DISCUSSIONHere's what a normal cilium is supposed to look like: a pair of central singlet microtubules, with nine—no more, no fewer—peripherally located doublet microtubules around it. One of each doublet pair has a "wing" on it that is the site of an ATPase, dynein, that splits ATP to provide the energy for movement.
This pattern of microtubules is found in all phyla of animals and it's not possible to tell from an image like this one whether the cilium is from a clam, a dog, or a human. It would appear that this arrangement is the only solution to the particular engineering problem involved in sliding some long, skinny tubules past each other in a controlled way. The image above is from a nasal biopsy from a different case, which was also suspected of being PCD.
Here's what Mr Peepers' biopsies looked like:
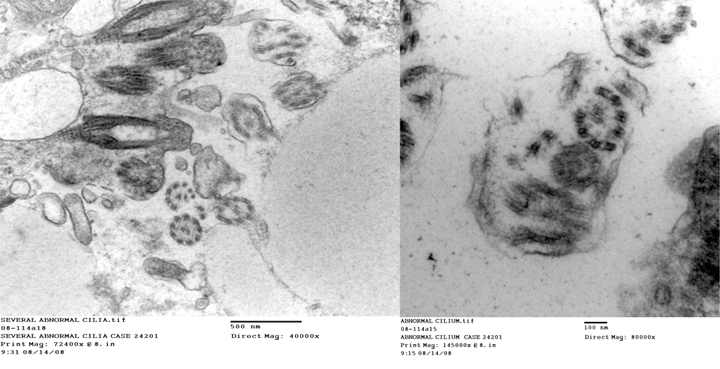
This pair of images shows several defective cilia: at left, in the low magnification picture, there is one in the center missing 2 pairs of doublets: at right, one is missing a doublet pair and at top right a few lonely doublets are present with no sign of any kind of normal organization. Here are some more images from this case:
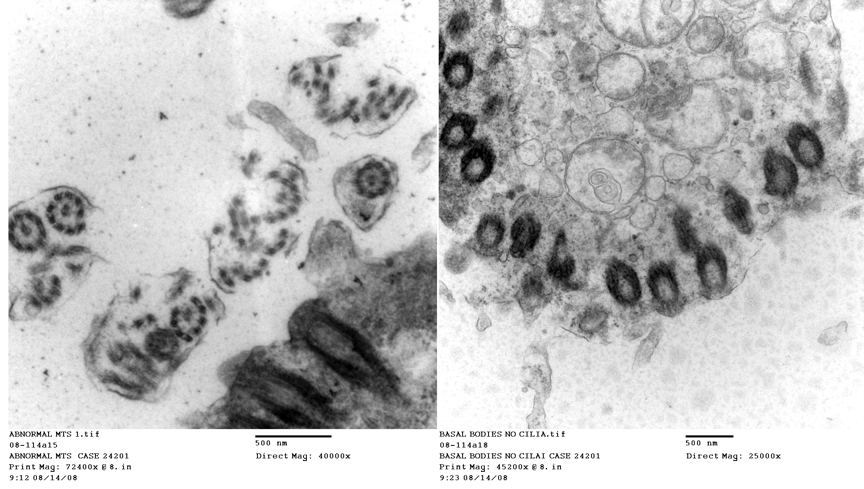
An even more deranged set of ciliary microtubules is seen at left: at right, the free surface of the cell has plenty of basal bodies (the "anchors" on which cilia rest) but no cilia at all!
Mr Peepers' problem is that he has a metabolic defect, a genetic mutation in the enzymes of pathways that control the normal synthesis and assembly of microtubules. What few cilia he has are non-functional because they're built wrong: if there ever were an example of how form and function are intertwined, PCD is it. Bad structure means poor to zero functionality. As is true of most genetic conditions, there are degrees of expression of the mutated genes: his littermate has PCD too, but a similar biopsy would show fewer affected cilia, hence his symptoms are less severe than Mr Peepers' are.
The cilia of the respiratory tract sweep particulate material trapped in the mucus layer up and outward by virtue of their directional beating. These cilia don't beat, hence an animal with PCD tends to get an accumulation of un-removed mucus and is prone to respiratory infections from opportunistic bacteria. Interference with gas exchange by mucus and low-grade inflammation cause distress on exercise, and in the very worst cases accumulated mucus causes severe and possibly fatal pneumonia.
There's no treatment for this except supportive measures. While antibiotics can keep the opportunistic infections down, that's not an answer. The brief respite they bring from the severe coughing and discharge are minor; this dog will have problems all his life, and likely will not have so long a life as an unaffected animal. That's also why he's so thin: he's balancing on the edge and will always be a "poor doer" as a result of his respiratory issues.
Oh, yes...the reason you have to use TEM is because while cilia are visible in the light microscope, microtubules aren't: they are well below the limit of resolution. Since this is really a case of defective microtubular synthesis, the initial clinical diagnosis has to be backed up with hard morphological evidence. Not all clients will pay for this sort of consult, but it's essential to understanding the true nature of the problem.