 The
cornea is the most important light-refracting structure of the eye. It produces
the initial image and casts it onto the lens behind it; the lens is in
turn responsible for accommodation of vision for different distance.
The
cornea is the most important light-refracting structure of the eye. It produces
the initial image and casts it onto the lens behind it; the lens is in
turn responsible for accommodation of vision for different distance.
The corneoscleral tunic can be divided into two general regions, the cornea and the sclera. They merge at the periphery of the cornea, in the region of the limbus of the eye.
The sclera is the tough collagenous bag which comprises the outer portion of the eye. It's composed mainly of collagen fibers oriented in all directions, but following the curve of the eyeball.
Its functions are to maintain the boundary of the eye; to serve as a protective envelope for the internal apparatus; and to provide a site of attachment of the muscles which move the eye up and down and from side to side. The sclera is also highly vascularized (since it is derived from the mesoderm of the head) and is a route for blood vessels and lymphatics. The venous drainage of the sclera carries the outflow of most of the eye's blood supply, and its lymphatic vessels carry off the excess aqueous humor. At its posterior aspect the optic nerve pierces the sclera; the epineurial covering of this nerve is continuous with the sclera and with the meninges of the brain.
The
cornea is the most important light-refracting structure of the eye. It produces
the initial image and casts it onto the lens behind it; the lens is in
turn responsible for accommodation of vision for different distance.
The curvature of the cornea is a major factor in the degree to which it refracts light coming into the eye, providing most of the focusing. Aberrations in the shape of the cornea have profound effects on vision, and surgical procedures to correct vision problems take advantage of this fact. It is possible to remove the cornea, alter its curvature; then stitch it back into place, with different focusing characteristics.
Because its embryonic origin is
from surface ectoderm, the cornea is avascular. Therefore it's physically isolated
from the blood circulatory system, and hence from the immune system. This situation
also has clinical implications. The "protected" nature of the cornea
makes it incapable of mounting a typical graft-rejection response, and corneal
transplants have a high rate of success.
LEFT:A diagrammatic representation of the cornea's layers.
 The
cornea is exposed to the environment on its outer surface, and is epithelial
in nature. The outermost part of the cornea is a stratified squamous layer,
the corneal epithelium. This layer isn't normally keratinized; it varies
in thickness among different species. The corneal epithelium is continuous at
its margins with the conjunctiva of the eyelids
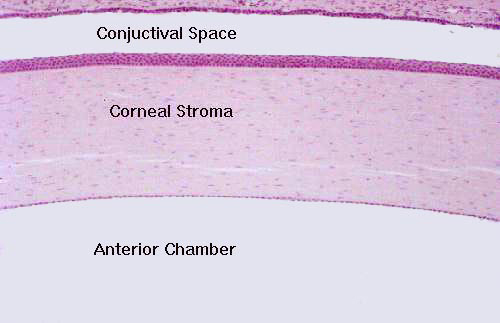
and the eyeball. At left is an image taken from an actual specimen. Compare
it to the diagram above. The cells of the corneal epithelium
sit on a thick basal lamina, Bowman's membrane, (named for Sir William Bowman,
1816-1892, the English ophthalmologist, anatomist and physiologist). The
inner surface of the cornea, demarcating the limit of the eye's anterior
chamber has a very thin, single layer of corneal endothelium. This
is a row of cuboidal cells. Between it and the substantia propria you
will find Descemet's membrane the basal lamina of the endothelial cells
(after Jean Descemet, 1732-1810, a French physician).
The
cornea is exposed to the environment on its outer surface, and is epithelial
in nature. The outermost part of the cornea is a stratified squamous layer,
the corneal epithelium. This layer isn't normally keratinized; it varies
in thickness among different species. The corneal epithelium is continuous at
its margins with the conjunctiva of the eyelids
and the eyeball. At left is an image taken from an actual specimen. Compare
it to the diagram above. The cells of the corneal epithelium
sit on a thick basal lamina, Bowman's membrane, (named for Sir William Bowman,
1816-1892, the English ophthalmologist, anatomist and physiologist). The
inner surface of the cornea, demarcating the limit of the eye's anterior
chamber has a very thin, single layer of corneal endothelium. This
is a row of cuboidal cells. Between it and the substantia propria you
will find Descemet's membrane the basal lamina of the endothelial cells
(after Jean Descemet, 1732-1810, a French physician).
The bulk of the tissue in the cornea is the substantia propria, a thick collagenous CT in the form of regular lamellae. The regular arrangement of these fibers gives the cornea its refractile properties.
Click Back to return
Or Go To:
Main Page | Corneoscleral Tunic | Uveal Tunic | Retinal Tunic | Physiology of Vision | CNS Processing of Visual Signals